11e posterior association cortex
•Download as PPT, PDF•
0 likes•7 views

The document discusses several key areas of the brain involved in sensory processing and integration. It describes how the somatosensory cortex integrates tactile and proprioceptive information, and how the posterior parietal cortex projects to motor areas. It also discusses pathways to visual, auditory and association areas, and how unimodal inputs converge on multimodal areas, allowing for comprehension, cognition and consciousness.

More Related Content
What's hot
What's hot (19)
Viewers also liked
Viewers also liked (20)
Similar to 11e posterior association cortex
Similar to 11e posterior association cortex (20)
More from PS Deb
More from PS Deb (20)
Recently uploaded
Recently uploaded (20)
11e posterior association cortex
- 4. Sensory Cortex Receptive Field
- 6. Columnar organization of somatosensory cortex
- 8. Association Cortex Information Flow
- 10. Pattern of Vibration of the Basilar Membrane
- 12. Discrimination of Sound “Patterns” by the Auditory Cortex
- 13. Pathways to the somatosensory, visual, and auditory association areas
- 14. Visual Pathway
- 16. Pathways to the somatosensory, visual, and auditory association areas
- 17. Unimodal sensory inputs converge on multimodal association areas
- 18. Interaction Among Association Areas Leads to Comprehension, Cognition, and Consciousness
- 20. Parietal Lobe
- 23. “ Attention Neurons” in the Monkey Parietal Cortex
- 24. Attention activity of Right Parietal Cortex in Normal
- 26. Temporal Lobe
- 33. Selective activation of face cells in the inferior temporal cortex of a rhesus monkey
- 34. Prosopognosia
- 35. Occipital Lobe
- 41. Thank You
Editor's Notes
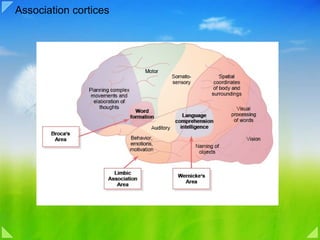
- Association Areas Figure 57–4 also shows several large areas of the cerebral cortex that do not fit into the rigid categories of primary and secondary motor and sensory areas. These areas are called association areas because they receive and analyze signals simultaneously from multiple regions of both the motor and sensory cortices as well as from subcortical structures. Yet even the association areas have their specializations. The most important association areas are (1) the parieto-occipitotemporal association area , (2) the prefrontal association area , and (3) the limbic association area . Following are explanations of the functions of these areas. Parieto-occipitotemporal Association Area. This association area lies in the large parietal and occipital cortical space bounded by the matosensory cortex anteriorly, the visual cortex posteriorly, and the auditory cortex laterally. As would be expected, it provides a high level of interpretative meaning for signals from all the surrounding sensory areas. However, even the parieto-occipitotemporal association area has its own functional subareas, which are shown in Figure 57–5. 1. Analysis of the Spatial Coordinates of the Body. An area beginning in the posterior parietal cortex and extending into the superior occipital cortex provides continuous analysis of the spatial coordinates of all parts of the body as well as of the surroundings of the body. This area receives visual sensory information from the posterior occipital cortex and simultaneous somatosensory information from the anterior parietal cortex. From all this information, it computes the coordinates of the visual, auditory, and body surroundings. 2. Area for Language Comprehension. The major area for language comprehension, called Wernicke ’ s area , lies behind the primary auditory cortex in the posterior part of the superior gyrus of the temporal lobe . We discuss this area much more fully later; it is the most important region of the entire brain for higher intellectual function because almost all such intellectual functions are language based. 3. Area for Initial Processing of Visual Language (Reading). Posterior to the language comprehension area, lying mainly in the anterolateral region of the occipital lobe, is a visual association area that feeds visual information conveyed by words read from a book into Wernicke’s area, the language comprehension area. This so-called angular gyrus area is needed to make meaning out of the visually perceived words. In its absence, a person can still have excellent language comprehension through hearing but not through reading. 4. Area for Naming Objects. In the most lateral portions of the anterior occipital lobe and posterior temporal lobe is an area for naming objects. The names are learned mainly through auditory input, whereas the physical natures of the objects are learned mainly through visual input. In turn, the names are essential for both auditory and visual language comprehension ( functions performed in Wernicke ’ s area located immediately superior to the auditory “names” region and anterior to the visual word processing area). Prefrontal Association Area. In Chapter 56, we learned that the prefrontal association area functions in close association with the motor cortex to plan complex patterns and sequences of motor movements. To aid in this function, it receives strong input through a massive subcortical bundle of nerve fibers connecting the parieto-occipitotemporal association area with the prefrontal association area. Through this bundle, the prefrontal cortex receives much preanalyzed sensory information, especially information on the spatial coordinates of the body that is necessary for planning effective movements. Much of the output from the prefrontal area into the motor control system passes through the caudate portion of the basal gangliathalamic feedback circuit for motor planning, which provides many of the sequential and parallel components of movement stimulation. The prefrontal association area is also essential to carrying out “ thought ” processes in the mind .This presumably results from some of the same capabilities of the prefrontal cortex that allow it to plan motor activities. It seems to be capable of processing non motor as well as motor information from widespread areas of the brain and therefore to achieve non motor types of thinking as well as motor types. In fact, the prefrontal association area is frequently described simply as important for elaboration of thoughts , and it is said to store on a short-term basis “working memories” that are used to combine new thoughts while they are entering the brain. Chapter 57 Cerebral Cortex, Intellectual Functions of the Brain, Learning and Memory 717 Broca’s Area. A special region in the frontal cortex, called Broca ’ s area , provides the neural circuitry for word formation . This area, shown in Figure 57–5, is located partly in the posterior lateral prefrontal cortex and partly in the premotor area. It is here that plans and motor patterns for expressing individual words or even short phrases are initiated and executed. This area also works in close association with Wernicke’s language comprehension center in the temporal association cortex, as we discuss more fully later in the chapter. An especially interesting discovery is the following: When a person has already learned one language and then learns a new language, the area in the brain where the new language is stored is slightly removed from the storage area for the first language. If both languages are learned simultaneously, they are stored together in the same area of the brain. Limbic Association Area. Figures 57–4 and 57–5 show still another association area called the limbic association area. This area is found in the anterior pole of the temporal lobe, in the ventral portion of the frontal lobe, and in the cingulate gyrus lying deep in the longitudinal fissure on the midsurface of each cerebral hemisphere. It is concerned primarily with behavior, emotions, and motivation. We will learn in Chapter 58 that the limbic cortex is part of a much more extensive system, the limbic system, that includes a complex set of neuronal structures in the midbasal regions of the brain. This limbic system provides most of the emotional drives for activating other areas of the brain and even provides motivational drive for the process of learning itself. Area for Recognition of Faces An interesting type of brain abnormality called prosophenosia is inability to recognize faces. This occurs in people who have extensive damage on the medial undersides of both occipital lobes and along the medioventral surfaces of the temporal lobes, as shown in Figure 57–6. Loss of these face recognition areas, strangely enough, results in little other abnormality of brain function. One wonders why so much of the cerebral cortex should be reserved for the simple task of face recognition. Most of our daily tasks involve associations Naming of objects Vision Visual processing of words Spatial coordinates of body and surroundings Somatosensory The occipital portion of this facial recognition area is contiguous with the visual cortex, and the temporal portion is closely associated with the limbic system that has to do with emotions, brain activation, and control of one’s behavioral response to the environment, as we see in Chapter 58. Word formation Broca‘s Area Limbic Association Area Wernicke‘s Area Auditory Behavior, emotions, motivation Language comprehension intelligence Motor Planning complex movements and elaboration of thoughts Figure 57–5 Map of specific functional areas in the cerebral cortex, showing especially Wernicke’s and Broca’s areas for language comprehension and speech production, which in 95 per cent of all people are located in the left hemisphere. 718 Unit XI The Nervous System: C. Motor and Integrative Neurophysiology
- Tactile Information About an Object is Fragmented by Peripheral Sensors and Must Be Integrated by the Brain The ability to recognize objects placed in the hand on the basis of touch alone is one of the most important and complex functions of the somatosensory system. By holding an object in the hand we can perceive its size, shape, texture, mass, and temperature. These properties together give rise to the percept of a coherent object. Neurologists call the ability to perceive form through touch stereognosis. Stereognosis not only tests the ability of the dorsal column-medial lemniscal system to transmit sensations from the hand but also measures the ability of cognitive processes in the brain to integrate that information. Many familiar objects such as an apple, a screwdriver, or a set of keys are much larger than the receptive field of any one receptor in the hand. These objects stimulate a large population of sensory nerve fibers, each of which scans a small portion of the object. The peripheral sensory apparatus deconstructs the object into tiny segments because, as we saw in Chapter 22, a sensory nerve fiber conveys information from only a small area of the receptor sheet. When a particular nerve fiber fires an action potential, it signals that its territory has been contacted at an intensity sufficient to cause it to fire. By analyzing which nerve fibers have been excited, the brain reconstructs the pattern made by the object. In addition, objects excite more than one kind of receptor. For example, a textured surface such as an array of Braille dots stimulates Merkel disk receptors, Meissner's corpuscles, and Pacinian corpuscles but evokes a different discharge pattern in each type of receptor because each signals a special feature of the stimulus. Similarly, the shape of an object is signaled by the firing patterns of Merkel disk receptors, which sense the curvature of the object's surface; by Meissner's corpuscles, which signal edges (where the curvature changes abruptly); and by the postural information provided by receptors in the muscles and joints of the hand. Thus, no single sensory axon, or even class of sensory axons, signals all of the relevant information. Spatial properties are processed by populations of receptors that form many parallel pathways to the brain. It is the job of the central nervous system to construct a coherent image of an object from fragmented information conveyed in multiple pathways. In this chapter we shall examine how neural circuits in the dorsal column-medial lemniscal system and the somatosensory areas of the cerebral cortex integrate information from neighboring areas of skin and different populations of receptors in order to form a percept.
- Figure 9.8. Somatotopic order in the human primary somatic sensory cortex. (A) Diagram showing the region of the human cortex from which electrical activity is recorded following mechanosensory stimulation of different parts of the body. The patients in the study were undergoing neurosurgical procedures for which such mapping was required. Although modern imaging methods are now refining these classical data, the human somatotopic map first defined in the 1930s has remained generally valid. (B) Diagram along the plane in (A) showing the somatotopic representation of body parts from medial to lateral. (C) Cartoon of the homunculus constructed on the basis of such mapping. Note that the amount of somatic sensory cortex devoted to the hands and face is much larger than the relative amount of body surface in these regions. A similar disproportion is apparent in the primary motor cortex, for much the same reasons (see Chapter 17 ). (After Penfield et al., 1953, and Corsi, 1991.) The Somatic Sensory Cortex The axons arising from neurons in the ventral posterior complex of the thalamus project to cortical neurons located primarily in layer IV of the somatic sensory cortex (see Figure 9.7 ; also see Box A in Chapter 26 for a more detailed description of cortical lamination). The somatic sensory cortex in humans, which is located in the parietal lobe, comprises four distinct regions, or fields, known as Brodmann's areas 3a, 3b, 1 , and 2 . Although area 3b is generally known as the primary somatic sensory cortex (also called SI), all four areas are involved in processing tactile information. Experiments carried out in nonhuman primates indicate that neurons in areas 3b and 1 respond primarily to cutaneous stimuli, whereas neurons in 3a respond mainly to stimulation of proprioceptors; area 2 neurons process both tactile and proprioceptive stimuli. Mapping studies in humans and other primates show further that each of these four cortical areas contains a separate and complete representation of the body. In these somatotopic maps , the foot, leg, trunk, forelimbs, and face are represented in a medial to lateral arrangement, as shown in Figures 9.8A , B and 9.9 . Although the topographic organization of the several somatic sensory areas is similar, the functional properties of the neurons in each region and their organization are distinct ( Box D ). For instance, the neuronal receptive fields are relatively simple in area 3b; the responses elicited in this region are generally to stimulation of a single finger. In areas 1 and 2, however, the majority of the receptive fields respond to stimulation of multiple fingers. Furthermore, neurons in area 1 respond preferentially to particular directions of skin stimulation, whereas many area 2 neurons require complex stimuli to activate them (such as a particular shape). Lesions restricted to area 3b produce a severe deficit in both texture and shape discrimination. In contrast, damage confined to area 1 affects the ability of monkeys to perform accurate texture discrimination. Area 2 lesions tend to produce deficits in finger coordination, and in shape and size discrimination. A salient feature of cortical maps, recognized soon after their discovery, is their failure to represent the body in actual proportion. When neurosurgeons determined the representation of the human body in the primary sensory (and motor) cortex, the homunculus (literally, “little man”) defined by such mapping procedures had a grossly enlarged face and hands compared to the torso and proximal limbs ( Figure 9.8C ). These anomalies arise because manipulation, facial expression, and speaking are extraordinarily important for humans, requiring more central (and peripheral) circuitry to govern them. Thus, in humans, the cervical spinal cord is enlarged to accommodate the extra circuitry related to the hand and upper limb, and as stated earlier, the density of receptors is greater in regions such as the hands and lips. Such distortions are also apparent when topographical maps are compared across species. In the rat brain, for example, an inordinate amount of the somatic sensory cortex is devoted to representing the large facial whiskers that provide a key component of the somatic sensory input for rats and mice (see Boxes B and D ), while raccoons overrepresent their paws and the platypus its bill. In short, the sensory input (or motor output) that is particularly significant to a given species gets relatively more cortical representation. Patterns of Organization within the Sensory Cortices: Brain Modules Observations over the last 40 years have made it clear that there is an iterated substructure within the somatic sensory (and many other) cortical maps. This substructure takes the form of units called modules , each involving hundreds or thousands of nerve cells in repeating patterns. The advantages of these iterated patterns for brain function remain largely mysterious; for the neurobiologist, however, such iterated arrangements have provided important clues about cortical connectivity and the mechanisms by which neural activity influences brain development (see Chapters 23 and 24 ). The observation that the somatic sensory cortex comprises elementary units of vertically linked cells was first noted in the 1920s by the Spanish neuroanatomist Rafael Lorente de Nó, based on his studies in the rat. The potential importance of cortical modularity remained largely unexplored until the 1950s, however, when electrophysiological experiments indicated an arrangement of repeating units in the brains of cats and, later, monkeys. Vernon Mountcastle, a neurophysiologist at Johns Hopkins, found that vertical microelectrode penetrations in the primary somatosensory cortex of these animals encountered cells that responded to the same sort of mechanical stimulus presented at the same location on the body surface. Soon after Mountcastle's pioneering work, David Hubel and Torsten Wiesel discovered a similar arrangement in the cat primary visual cortex. These and other observations led Mountcastle to the general view that “the elementary pattern of organization of the cerebral cortex is a vertically oriented column or cylinder of cells capable of input-output functions of considerable complexity.” Since these discoveries in the late 1950s and early 1960s, the view that modular circuits represent a fundamental feature of the mammalian cerebral cortex has gained wide acceptance, and many such entities have now been described in various cortical regions (see figure). This wealth of evidence for patterned circuits has led many neuroscientists to conclude, like Mountcastle, that modules are a fundamental feature of the cerebral cortex, essential for perception, cognition, and perhaps even consciousness. Despite the prevalence of iterated modules, there are some problems with the view that modular units are universally important in cortical function. First, although modular circuits of a given class are readily seen in the brains of some species, they have not been found in other, sometimes closely related, animals. Second, not all regions of the mammalian cortex are organized in a modular fashion. And third, no clear function of such modules has been discerned, much effort and speculation notwithstanding. This salient feature of the organization of the somatic sensory cortex and other cortical (and some subcortical) regions therefore remains a tantalizing puzzle.
- Figure 22-5 Two-point discrimination varies throughout the body surface. The two-point threshold measures the minimum distance at which two stimuli are resolved as distinct. At smaller separations the stimuli are blurred into a single continuous sensation spanning the distance between the points. Two-point thresholds are measured clinically using a calibrated compass in which the separation of the tips is accurately scaled. Two-point thresholds can also be determined from measurements of the ability of subjects to discriminate the orientation of grating ridges as a function of their spacing. This method measures spatial acuity more accurately. The two-point threshold varies for different body regions; it is about 2 mm on the finger tip but increases to 10 mm on the palm and 40 mm on the arm. The two-point thresholds highlighted in pink match the diameter of the corresponding receptive fields shown in pink on the body. The greatest discriminative capacity is afforded in the finger tips, lips, and tongue, which have the smallest receptive fields. (Adapted from Weinstein 1968.) The size of the receptive fields in a particular region of skin delimits the capacity to determine whether one or more points are stimulated. A sensory neuron innervating Meissner's corpuscles and Merkel disk receptors transmits information about the largest skin indentation within its receptive field. If two points within the same receptive field are stimulated, the neuron will signal only the larger indentation. But if the points are located in the receptive fields of two different nerve fibers, then information about both points of stimulation will be signaled. The farther apart the points lie on the surface, the greater the likelihood that the two active nerves will be separated by silent nerve fibers. The contrast between active and inactive nerve fibers seems to be necessary for resolving spatial detail. Spatial resolution of stimuli on various regions of the skin can be quantified in humans by measuring their ability to perceive a pair of nearby stimuli as two distinct entities. The minimum distance between two detectable stimuli is called the two-point threshold. The twopoint threshold varies for different body regions (Figure 22-5). These variations are correlated with the size of sensory receptive fields and the innervation density of mechanoreceptors in the superficial layers of the skin. Thus, measurements of sensory function of the human hand reveal important information concerning the organization of peripheral sense organs. Differences in Mechanosensory Discrimination Across the Body Surface The accuracy with which tactile stimuli can be sensed varies from one region of the body to another, a phenomenon that illustrates some further principles of somatic sensation. Figure 9.4 shows the results of an experiment in which variation in tactile ability across the body surface was measured by two-point discrimination . This technique measures the minimal interstimulus distance required to perceive two simultaneously applied stimuli as distinct (the indentations of the points of a pair of calipers, for example). When applied to the skin, such stimuli of the fingertips are discretely perceived if they are only 2 mm apart. In contrast, the same stimuli applied to the forearm are not perceived as distinct until they are at least 40 mm apart! This marked regional difference in tactile ability is explained by the fact that the encapsulated mechanoreceptors that respond to the stimuli are three to four times more numerous in the fingertips than in other areas of the hand, and many times more dense than in the forearm. Equally important in this regional difference are the sizes of the neuronal receptive fields. The receptive field of a somatic sensory neuron is the region of the skin within which a tactile stimulus evokes a sensory response in the cell or its axon ( Boxes A and B ). Analysis of the human hand shows that the receptive fields of mechanosensory neurons are 1–2 mm in diameter on the fingertips but 5–10 mm on the palms. The receptive fields on the arm are larger still. The importance of receptive field size is easy to envision. If, for instance, the receptive fields of all cutaneous receptor neurons covered the entire digital pad, it would be impossible to discriminate two spatially separate stimuli applied to the fingertip (since all the receptive fields would be returning the same spatial information). Receptor density and receptive field sizes in different regions are not the only factors determining somatic sensation. Psychophysical analysis of tactile performance suggests that something more than the cutaneous periphery is needed to explain variations in tactile perception. For instance, sensory thresholds in two-point discrimination tests vary with practice, fatigue, and stress. The contextual significance of stimuli is also important in determining what we feel; even though we spend most of the day wearing clothes, we usually ignore the tactile stimulation that they produce. Some aspect of the mechanosensory system allows us to filter out this information and pay attention to it only when necessary. The fascinating phenomenon of “phantom limb” sensations after amputation (see Box B in Chapter 10 ) provides further evidence that tactile perception is not fully explained by the peripheral information that travels centrally. The central nervous system clearly plays an active role in determining the perception of the mechanical forces that act on us
- Figure 26 - 11 Columnar organization of somatosensory cortex. Diagram illustrates that different fingers (D1 - D3) are represented on adjoining regions of somatosensory cortex. Within the area represented by each finger, there are alternating columns of neurons that are rapidly adapting (green) and slowly adapting (red). The inputs for each type of receptor for each digit are organized into separate columns. (From Bear MF, et al.: Neuroscience: Exploring the Brain, 2nd ed. Philadelphia: Lippincott Williams & Wilkins, The Parietal Lobe The principal unit of organization is the cortical column ( Fig. 26 - 11 ). Within each column, neurons located in each of the layers within a given column respond best to a single class of receptors, and all of the neurons respond to stimulation applied to the same local region of the body surface ( Fig. 26 - 11 ). Adjoining columns representing the same body surface have different physiological properties, such as being rapidly adapting or slowly adapting to sensory stimulation. Other characteristics concerning somatosensory neurons should also be noted. For example, as indicated earlier, different regions of the somatosensory cortex may respond to different modalities of stimulation, but they also have a preference for responding to a single type of stimulus. Like other sensory modalities, certain classes of somatosensory neurons appear to respond to complex aspects of a given form of stimulation. For example, although one class of neurons may respond to any form of tactile stimulation applied to a certain region of the body surface, other more complex neurons may respond to the orientation and direction of stimulation. Such response properties suggest that these neurons have larger receptor fields and are capable of integrating the activities of other more basic neurons located in a slightly different region of somatosensory cortex. In fact, it is suggested that the neurons that respond to the more simple aspects of stimulation lie in the region of area 3 and the neurons that respond to the more complex properties of stimulation lie in area 2. It is the increased complexity of the response properties of these neurons that likely provides the neuronal basis for spatial perception that is essential for recognition of three - dimensional objects (i.e., stereognosis). It is important to note that such perceptual discriminations are essential for complex skilled movements to be made.
- Figure 23-1 The somatic sensory cortex has three major divisions: the primary and secondary somatosensory cortices and the posterior parietal cortex. A. The anatomical location of the three divisions of the somatic sensory cortex is seen best from a lateral perspective of the surface of the cerebral cortex. The primary somatic sensory cortex (S-I) forms the most rostral portion of the parietal lobe. It covers the postcentral gyrus, beginning at the bottom of the central sulcus and extending posteriorly to the postcentral and intraparietal sulci. The postcentral gyrus also extends into the medial wall of the hemisphere to the cingulate gyrus. The posterior parietal cortex (Brodmann's areas 5 and 7) lies immediately posterior to S-I. The secondary somatic sensory cortex (S-II) is located on the parietal operculum of the lateral sulcus (fissure of Sylvius). B. The relationship of the S-I to the S-II cortex is illustrated in a coronal section through the cortex. The S-II cortex lies lateral to S-I, and extends laterally to the insular cortex, forming the superior bank of the lateral sulcus. The numbers on the section indicate Brodmann's cytoarchitectural areas. C. S-I is subdivided into four distinct cytoarchitectonic regions (Brodmann's areas). This sagittal section illustrates the spatial relationship of these four regions to area 5 of the posterior parietal cortex. Somatosensory input to the cortex originates from the ventral posterior lateral nucleus of the thalamus. Neurons in this nucleus project to all areas in S-I, mainly to Brodmann's areas 3a and 3b but also to areas 1 and 2. In turn, neurons in areas 3a and 3b project to areas 1 and 2, and all of these project to S-II and to posterior parietal cortex. These higher-order somatosensory areas also contain distinct cytoarchitectonic and functional subregions that are not illustrated here. (Modified from Jones and Friedman 1982.) The Primary Somatic Sensory Cortex Integrates Information About Touch The anatomical plan of the somatic sensory system reflects an organizational principle common to all sensory systems: Sensory information is processed in a series of relay regions within the brain. We learned in Chapter 22 that there are only three synaptic relay sites between sensory receptors in the skin and the cerebral cortex (see Figure 22-14). Mechanoreceptors in the skin send their axons to the caudal medulla, where they terminate in the gracile or cuneate nuclei. These second-order neurons project directly to the contralateral thalamus, terminating in the ventral posterior lateral nucleus. A parallel pathway from the principal trigeminal nucleus, which represents the face, ascends to the ventral posterior medial nucleus. The third-order neurons in the thalamus send axons to the primary somatic sensory cortex (S-I), located in the postcentral gyrus of the parietal lobe. As we learned in Chapter 20, the primary somatic cortex S-I contains four cytoarchitectural areas: Brodmann's areas 3a, 3b, 1, and 2 (Figure 23-1). Most thalamic fibers terminate in areas 3a and 3b, and the cells in areas 3a and 3b project their axons to areas 1 and 2. Thalamic neurons also send a small projection directly to Brodmann's areas 1 and 2. These four regions of the cortex differ functionally. Areas 3b and 1 receive information from receptors in the skin, whereas areas 3a and 2 receive proprioceptive information from receptors in muscles and joints. However, the four areas of the cortex are extensively interconnected, so that both serial and parallel processing are involved in higher-order elaboration of sensory information. The secondary somatic sensory cortex (S-II), located on the superior bank of the lateral fissure, is innervated by neurons from each of the four areas of S-I (Figure 23-1C). The projections from S-I are required for the function of S-II. For example, when the neural connections from the hand area of S-I are removed, stimuli applied to the skin of the hand do not activate neurons in S-II. In contrast, removal of parts of S-II has no effect on the response of neurons in S-I. The S-II cortex projects to the insular cortex , which in turn innervates regions of the temporal lobe believed to be important for tactile memory. Finally, as we have seen in Chapters 19 and 20, other important somatosensory cortical areas are located in the posterior parietal cortex (Brodmann's areas 5 and 7). These areas receive input from S-I as well as input from the pulvinar and thus have an associational function. They are also connected bilaterally through the corpus callosum. Area 5 integrates tactile information from mechanoreceptors in the skin with proprioceptive inputs from the underlying muscles and joints. This region also integrates information from the two hands. Area 7 receives visual as well as tactile and proprioceptive inputs, allowing integration of stereognostic and visual information. The posterior parietal cortex projects to the motor areas of the frontal lobe and plays an important role in sensory initiation and guidance of movement.
- Monaural Pathways from the Cochlear Nucleus to the Lateral Lemniscus The binaural pathways for sound localization are only part of the output of the cochlear nucleus. This fact is hardly surprising, given that auditory perception involves much more than locating the position of the sound source. A second major set of pathways from the cochlear nucleus bypasses the superior olive and terminates in the nuclei of the lateral lemniscus on the contralateral side of the brainstem (see Figure 13.11 ). These particular pathways respond to sound arriving at one ear only and are thus referred to as monaural. Some cells in the lateral lemniscus nuclei signal the onset of sound, regardless of its intensity or frequency. Other cells in the lateral lemniscus nuclei process other temporal aspects of sound, such as duration. The precise role of these pathways in processing temporal features of sound is not yet known. As with the outputs of the superior olivary nuclei, the pathways from the nuclei of the lateral lemniscus converge at the midbrain. Integration in the Inferior Colliculus Auditory pathways ascending via the olivary and lemniscal complexes, as well as other projections that arise directly from the cochlear nucleus, project to the midbrain auditory center, the inferior colliculus (see Figure 13.11 ). In examining how integration occurs in the inferior colliculus, it is again instructive to turn to the most completely analyzed auditory mechanism, the binaural system for localizing sound. As already noted, space is not mapped on the auditory receptor surface; thus the perception of auditory space must somehow be synthesized by circuitry in the lower brainstem and midbrain. Experiments in the barn owl, an extraordinarily proficient animal at localizing sounds, show that the convergence of binaural inputs in the midbrain produces something entirely new relative to the periphery—namely, a computed topographical representation of auditory space. Neurons within this auditory space map in the colliculus respond best to sounds originating in a specific region of space and thus have both a preferred elevation and a preferred horizontal location, or azimuth. Although comparable maps of auditory space have not yet been found in mammals, humans have a clear perception of both the elevational and azimuthal components of a sound's location, suggesting that we have a similar auditory space map. Another important property of the inferior colliculus is its ability to process sounds with complex temporal patterns. Many neurons in the inferior colliculus respond only to frequency-modulated sounds, while others respond only to sounds of specific durations. Such sounds are typical components of biologically relevant sounds, such as those made by predators, or intraspecific communication sounds, which in humans include speech. The inferior colliculus is evidently the first stage in a system, continued in the auditory thalamus and cortex, that analyzes sounds that have particular significance. The Auditory Thalamus Despite the parallel pathways in the auditory stations of the brainstem and midbrain, the medial geniculate complex ( MGC ) in the thalamus is an obligatory relay for all ascending auditory information destined for the cortex (see Figure 13.11). Most input to the MGC arises from the inferior colliculus, although a few auditory axons from the lower brainstem bypass the inferior colliculus to reach the auditory thalamus directly. The MGC has several divisions, including the ventral division, which functions as the major thalamocortical relay, and the dorsal and medial divisions, which are organized like a belt around the ventral division. In some mammals, the strictly maintained tonotopy of the lower brainstem areas is exploited by convergence onto MGC neurons, generating specific responses to certain spectral combinations. The original evidence for this statement came from research on the response properties of cells in the MGC of echolocating bats. Some cells in the so-called belt areas of the bat MGC respond only to combinations of widely spaced frequencies that are specific components of the bat's echolocation signal and of the echoes that are reflected from objects in the bat's environment. In the mustached bat, where this phenomenon has been most thoroughly studied, the echolocation pulse has a changing frequency (frequency-modulated, or FM) component that includes a fundamental frequency and one or more harmonics. The fundamental frequency (FM1) has low intensity and sweeps from 30 kHz to 20 kHz. The second harmonic (FM2) is the most intense component and sweeps from 60 kHz to 40 kHz. Note that these frequencies do not overlap. Most of the echoes are from the intense FM2 sound, and virtually none arise from the weak FM1, even though the emitted FM1 is loud enough for the bat to hear. Apparently, the bat assesses the distance to an object by measuring the delay between the FM1 emission and the FM2 echo. Certain MGC neurons respond when FM2 follows FM1 by a specific delay, providing a mechanism for sensing such frequency combinations. Because each neuron responds best to a particular delay, a range of distances is encoded by the population of MGC neurons. Bat sonar illustrates two important points about the function of the auditory thalamus. First, the MGC is the first station in the auditory pathway where selectivity for combinations of frequencies is found. The mechanism responsible for this selectivity is presumably the ultimate convergence of inputs from cochlear areas with different spectral sensitivities. Second, cells in the MGC are selective not only for frequency combinations, but also for specific time intervals between the two frequencies. The principle is the same as that described for binaural neurons in the medial superior olive, but in this instance, two monaural signals with different frequency sensitivity coincide, and the time difference is in the millisecond rather than the microsecond range. In summary, neurons in the medial geniculate complex receive convergent inputs from spectrally and temporally separate pathways. This complex, by virtue of its convergent inputs, mediates the detection of specific spectral and temporal combinations of sounds. In many species, including humans, varying spectral and temporal cues are especially important features of communication sounds. It is not known whether cells in the human medial geniculate are selective to combinations of sounds, but the processing of speech certainly requires both spectral and temporal combination sensitivity.
- Figure 13.5. Traveling waves along the cochlea. A traveling wave is shown at a given instant along the cochlea, which has been uncoiled for clarity. The graphs profile the amplitude of the traveling wave along the basilar membrane for different frequencies and show that the position where the traveling wave reaches its maximum amplitude varies directly with the frequency of stimulation. (Drawing after Dallos, 1992; graphs after von Békésy, 1960.) Pattern of Vibration of the Basilar Membrane for Different Sound Frequencies. Note in Figure 52–5 the different patterns of transmission for sound waves of different frequencies. Each wave is relatively weak at the outset but becomes strong when it reaches that portion of the basilar membrane that has a natural resonant frequency equal to the respective sound frequency. At this point, the basilar membrane can vibrate back and forth with such ease that the energy in the wave is dissipated. Consequently, the wave dies at this point and fails to travel the remaining distance along the basilar membrane. Thus, a high-frequency sound wave travels only a short distance along the basilar membrane before it reaches its resonant point and dies, a medium-frequency sound wave travels about halfway and then dies, and a very low frequency sound wave travels the entire distance along the membrane. Another feature of the traveling wave is that it travels fast along the initial portion of the basilar membrane but becomes progressively slower as it goes farther into the cochlea. The cause of this is the high coefficient of elasticity of the basilar fibers near the oval window and a progressively decreasing coefficient farther along the membrane. This rapid initial transmission of the wave allows the high-frequency sounds to travel far enough into the cochlea to spread out and separate from one another on the basilar membrane. Without this, all the high-frequency waves would be bunched together within the first millimeter or so of the basilar membrane, and their frequencies could not be discriminated from one another.
- The Auditory Cortex Figure 13.14. The human auditory cortex. (A) Diagram showing the brain in left lateral view, including the depths of the lateral sulcus, where part of the auditory cortex occupying the superior temporal gyrus normally lies hidden. The primary auditory cortex (A1) is shown in blue; the surrounding belt areas of the auditory cortex are in red. (B) The primary auditory cortex has a tonotopic organization, as shown in this blowup diagram of a segment of A1. The ultimate target of afferent auditory information is the auditory cortex. Although the auditory cortex has a number of subdivisions, a broad distinction can be made between a primary area and peripheral, or belt, areas. The primary auditory cortex ( A1 ) is located on the superior temporal gyrus in the temporal lobe and receives point-to-point input from the ventral division of the medial geniculate complex; thus, it contains a precise tonotopic map. The belt areas of the auditory cortex receive more diffuse input from the belt areas of the medial geniculate complex and therefore are less precise in their tonotopic organization. The primary auditory cortex (A1) has a topographical map of the cochlea ( Figure 13.14 ), just as the primary visual cortex (V1) and the primary somatic sensory cortex (S1) have topographical maps of their respective sensory epithelia. Unlike the visual and somatic sensory systems, however, the cochlea has already decomposed the acoustical stimulus so that it is arrayed tonotopically along the length of the basilar membrane. Thus, A1 is said to comprise a tonotopic map, as do most of the ascending auditory structures between the cochlea and the cortex. Orthogonal to the frequency axis of the tonotopic map is a striped arrangement of binaural properties. The neurons in one stripe are excited by both ears (and are therefore called EE cells), while the neurons in the next stripe are excited by one ear and inhibited by the other ear (EI cells). The EE and EI stripes alternate, an arrangement that is reminiscent of the ocular dominance columns in V1 (see Chapter 12 ). The sorts of sensory processing that occur in the other divisions of the auditory cortex are not well understood, but they are likely to be important to higher-order processing of natural sounds, including those used for communication. It appears that some areas are specialized for processing combinations of frequencies, while others are specialized for processing modulations of amplitude or frequency. Sounds that are especially important for intraspecific communication often have a highly ordered temporal structure. In humans, the best example of such time-varying signals is speech, where different phonetic sequences are perceived as distinct syllables and words. Behavioral studies in cats and monkeys show that the auditory cortex is especially important for processing temporal sequences of sound. If the auditory cortex is ablated in these animals, they lose the ability to discriminate between two complex sounds that have the same frequency components but which differ in temporal sequence. Thus, without the auditory cortex, monkeys cannot discriminate one conspecific communication sound from another. Studies of human patients with bilateral damage to the auditory cortex also reveal severe problems in processing the temporal order of sounds. It seems likely, therefore, that specific regions of the human auditory cortex are specialized for processing elementary speech sounds, as well as other temporally complex acoustical signals, such as music. Indeed, Wernicke's area, which is critical to the comprehension of human language, lies within the secondary auditory area ( Figure 13.15 ; see also Chapter 27 ).
- Figure 13.15. The human auditory cortical areas related to processing speech sounds. (A) Diagram of the brain in left lateral view, showing locations in the intact hemisphere. (B) An oblique section (plane of dashed line in A) shows the cortical areas on the superior surface of the temporal lobe. Note that Wernicke's area, a region important in comprehending speech, is just posterior to the primary auditory cortex. Discrimination of Sound “Patterns” by the Auditory Cortex. Complete bilateral removal of the auditory cortex does not prevent a cat or monkey from detecting sounds or reacting in a crude manner to sounds. However, it does greatly reduce or sometimes even abolish the animal’s ability to discriminate different sound pitches and especially patterns of sound. For instance, an animal that has been trained to recognize a combination or sequence of tones, one following the other in a particular pattern, loses this ability when the auditory cortex is destroyed; furthermore, the animal cannot relearn this type of response. Therefore, the auditory cortex is especially important in the discrimination of tonal and sequential sound patterns. Destruction of both primary auditory cortices in the human being greatly reduces one’s sensitivity for hearing. Destruction of one side only slightly reduces hearing in the opposite ear; it does not cause deafness in the ear because of many crossover connections from side to side in the auditory neural pathway. However, it does affect one’s ability to localize the source of a sound, because comparative signals in both cortices are required for the localization function. Lesions that affect the auditory association areas but not the primary auditory cortex do not decrease a person’s ability to hear and differentiate sound tones or even to interpret at least simple patterns of sound. However, he or she is often unable to interpret the meaning of the sound heard. For instance, lesions in the posterior portion of the superior temporal gyrus, which is called Wernicke’s area and is part of the auditory association cortex, often make it impossible for a person to interpret the meanings of words even though he or she hears them perfectly well and can even repeat them. These functions of the auditory association areas and their relation to the overall intellectual functions of the brain are discussed in more detail in Chapter 57. Summary Sound waves are transmitted via the external and middle ear to the cochlea of the inner ear, which exhibits a traveling wave when stimulated. For high-frequency sounds, the amplitude of the traveling wave reaches a maximum at the base of the cochlea; for low-frequency sounds, the traveling wave reaches a maximum at the apical end. The associated motions of the basilar membrane are transduced primarily by the inner hair cells, while the basilar membrane motion is itself actively modulated by the outer hair cells. Damage to the outer or middle ear results in conductive hearing loss, while hair cell damage results in a sensorineural hearing deficit. The tonotopic organization of the cochlea is retained at all levels of the central auditory system. Projections from the cochlea travel via the eighth nerve to the three main divisions of the cochlear nucleus. The targets of the cochlear nucleus neurons include the superior olivary complex and nuclei of the lateral lemniscus, where the binaural cues for sound localization are processed. The inferior colliculus is the target of nearly all of the auditory pathways in the lower brainstem and carries out important integrative functions, such as processing sound frequencies and integrating the cues for localizing sound in space. The primary auditory cortex, which is also organized tonotopically, is essential for basic auditory functions, such as frequency discrimination and sound localization. The belt areas of the auditory cortex have a less strict tonotopic organization and probably process complex sounds, such as those that mediate communication. In the human brain, the major speech comprehension areas are located in the zone immediately adjacent to the auditory cortex
- Figure 19-3 Pathways to the somatosensory, visual, and auditory association areas. Connections between cortical areas represent stages of information processing. At each stage progressively more abstract information is extracted from the sensory stimulus. Sensory information flows from the primary sensory areas (orange = primary somatosensory cortex; purple = primary visual cortex; yellow = primary auditory cortex) to adjacent unimodal association cortex. (From Jones EG, Powell TPS. 1970. Brain 93:793-820) Three Principles Govern the Function of the Association Areas Studies of afferent sensory pathways and association areas in the cortex have led to three important principles of sensory information processing: Sensory information is processed in a series of relays along several parallel pathways from peripheral receptors through primary sensory cortex and unimodal association cortex to the multimodal association cortex of the posterior part of the hemisphere: the posterior parietal and temporal cortices. Sensory information representing different modalities converges upon areas of cortex that integrate that information into a polysensory event. The posterior association areas that process sensory information are highly interconnected with the frontal association areas responsible for planning motor actions. These anterior association areas convert plans about future behaviors to concrete motor responses, such as satisfying hunger by eating. Sensory Information Is Processed Both Sequentially and in Parallel Cortical processing of sensory information has been studied most extensively in the visual and somatosensory systems, but the general principles derived from these studies apply to the other sensory modalities as well. In the chapters on the visual system (Chapters 25,26,27,28,29) we shall examine the cortical mechanisms that process incoming sensory signals into coherent information to construct visual perceptions. We shall learn how the axons of neurons in the primary visual cortex conveying simple sensory information converge on cells in adjacent secondary visual areas (Figure 19-3). The secondary visual areas are unimodal association areas. Even though neurons in these areas respond selectively to an array of inputs and are able to signal more complex aspects of the visual image, the information they process is entirely visual. In the monkey specific neurons in the visual association areas of the temporal lobe respond preferentially to a particular complex shape, such as a hand; some may respond selectively to specific faces. Damage to secondary sensory areas or to unimodal association cortex impairs the processing of specific types of sensory information, a condition called agnosia (Greek, “not knowing”). Injury to ventral areas of extra-striate cortex in humans may destroy the ability to recognize objects presented visually without affecting the ability to identify the same object by touch ( apperceptive agnosia ). Some patients can perceive an object and draw it accurately but cannot name it ( associative agnosia ).
- Figure 28-2 The magnocellular (M) and parvocellular (P) pathways from the retina project through the lateral geniculate nucleus (LGN) to V1. Separate pathways to the temporal and parietal cortices course through the extrastriate cortex beginning in V2. The connections shown in the figure are based on established anatomical connections, but only selected connections are shown and many cortical areas are omitted (compare Figure 25- 9). Note the cross connections between the two pathways in several cortical areas. The parietal pathway receives input from the M pathway but only the temporal pathway receives input from both the M and P pathways. (Abbreviations: AIT = anterior inferior temporal area; CIT = central inferior temporal area; LIP = lateral intraparietal area; Magno = magnocellular layers of the lateral geniculate nucleus; MST = medial superior temporal area; MT = middle temporal area; Parvo = parvocellular layers of the lateral geniculate nucleus; PIT = posterior inferior temporal area; VIP = ventral intraparietal area.) (Based on Merigan and Maunsell 1993.) Margaret Livingstone and David Hubel identified the anatomical connections between labeled regions in V1 and V2 (Figure 28-1B). They found that the P and M pathways remain partially segregated through V2. The M pathway projects from the magnocellular layers of the lateral geniculate nucleus to the striate cortex, first to layer 4Cα and then to layer 4B. Cells in layer 4B project directly to the middle temporal area (MT) and also to the thick stripes in V2, from which cells also project to MT. Thus, a clear anatomical pathway exists from the magnocellular layers in the lateral geniculate nucleus to MT and from there to the posterior parietal cortex (Figure 28-2). Cells in the parvocellular layers of the lateral geniculate nucleus project to layer 4Cβ in the striate cortex, from which cells project to the blobs and interblobs of V1. The blobs send a strong projection to the thin stripes in V2, whereas interblobs send a strong projection to the interstripes in V2. The thin stripe and interstripe areas of V2 may in turn project to discrete subregions of V4, thus maintaining this separation in the P pathway into V4 and possibly on into the inferior temporal cortex. A pathway from the P cells in the lateral geniculate nucleus to the inferior temporal cortex can therefore also be identified (Figure 28-2). But are these pathways exclusive of each other? Several anatomical observations suggest that they are not. In V1 both the magnocellular and parvocellular pathways have inputs in the blobs, and local neurons make extensive connections between the blob and interblob compartments. In V2 cross connections exist between the stripe compartments. Thus, the separation is not absolute, but whether there is an intermixing of the M and P contributions or whether the cross connections allow one cortical pathway to modulate activity in the other is not clear. Results of experiments that selectively inactivate the P and M pathways as they pass through the lateral geniculate nucleus (described in Chapter 27) also erode the notion of strict segregation between the pathways in V1. Blocking of either pathway affects the responses of fewer than half the neurons in V1, which indicates that most V1 neurons receive physiologically effective inputs from both pathways. Further work has shown that the responses of neurons both within and outside of the blobs in the superficial layers of V1 are altered by blocking only the M pathway. Both observations suggest that there is incomplete segregation of the M and P pathways in V1. This selective blocking of the P and M pathways also reveals the relative contributions of the pathways to the parietal and inferior temporal cortices. Blocking the magnocellular layers of the lateral geniculate nucleus eliminates the responses of many cells in MT and always reduces the responses of the remaining cells; blocking the parvocellular layers produces a much weaker effect on cells in MT. In contrast, blocking the activity of either the parvocellular or magnocellular layers in the lateral geniculate nucleus reduces the activity of neurons in V4. Thus, the dorsal pathway to MT seems primarily to include input from the M pathway, whereas the ventral pathway to the inferior temporal cortex appears to include input from both the M and P pathways. We can now see that there is substantial segregation of the P and M pathways up to V1, probably separation into V2, a likely predominance of the M input to the dorsal pathway to MT and the parietal cortex, and a mixture of P and M input into the pathway leading to the inferior temporal lobe (as indicated by the lines crossing between the pathways in Figure 28-2). What should we conclude about the organization of visual processing throughout the multiple areas of the visual cortex? First, we know that there are specific serial pathways through the multiple visual areas, not just a random assortment of equally connected areas. There is substantial evidence for two major processing pathways, a dorsal one to the posterior parietal cortex and a ventral one to the inferior temporal cortex, but other pathways may also exist. Second, there is strong evidence that the processing in these two cortical pathways is hierarchical. Each level has strong projections to the next level (and projections back), and the type of visual processing changes systematically from one level to the next. Third, the functions of cortical areas in the two cortical pathways are strikingly different, as judged both by the anatomical connections and the cellular activity considered in this chapter and by the behavioral and brain imaging evidence discussed in Chapter 25. Our examination of the functional organization within these vast regions of extrastriate visual cortex begins with the dorsal cortical pathway and the most intensively studied visual attribute, motion. We then examine the processing of depth information in the dorsal pathway. Finally, we turn to the ventral cortical pathway and consider the processing of information related to form. Color vision is the subject of the next chapter.
- Figure 19-3 Pathways to the somatosensory, visual, and auditory association areas. Connections between cortical areas represent stages of information processing. At each stage progressively more abstract information is extracted from the sensory stimulus. Sensory information flows from the primary sensory areas (orange = primary somatosensory cortex; purple = primary visual cortex; yellow = primary auditory cortex) to adjacent unimodal association cortex. (From Jones EG, Powell TPS. 1970. Brain 93:793-820) Three Principles Govern the Function of the Association Areas Studies of afferent sensory pathways and association areas in the cortex have led to three important principles of sensory information processing: Sensory information is processed in a series of relays along several parallel pathways from peripheral receptors through primary sensory cortex and unimodal association cortex to the multimodal association cortex of the posterior part of the hemisphere: the posterior parietal and temporal cortices. Sensory information representing different modalities converges upon areas of cortex that integrate that information into a polysensory event. The posterior association areas that process sensory information are highly interconnected with the frontal association areas responsible for planning motor actions. These anterior association areas convert plans about future behaviors to concrete motor responses, such as satisfying hunger by eating. Sensory Information Is Processed Both Sequentially and in Parallel Cortical processing of sensory information has been studied most extensively in the visual and somatosensory systems, but the general principles derived from these studies apply to the other sensory modalities as well. In the chapters on the visual system (Chapters 25,26,27,28,29) we shall examine the cortical mechanisms that process incoming sensory signals into coherent information to construct visual perceptions. We shall learn how the axons of neurons in the primary visual cortex conveying simple sensory information converge on cells in adjacent secondary visual areas (Figure 19-3). The secondary visual areas are unimodal association areas. Even though neurons in these areas respond selectively to an array of inputs and are able to signal more complex aspects of the visual image, the information they process is entirely visual. In the monkey specific neurons in the visual association areas of the temporal lobe respond preferentially to a particular complex shape, such as a hand; some may respond selectively to specific faces. Damage to secondary sensory areas or to unimodal association cortex impairs the processing of specific types of sensory information, a condition called agnosia (Greek, “not knowing”). Injury to ventral areas of extra-striate cortex in humans may destroy the ability to recognize objects presented visually without affecting the ability to identify the same object by touch ( apperceptive agnosia ). Some patients can perceive an object and draw it accurately but cannot name it ( associative agnosia ).
- Figure 19-4 Unimodal sensory inputs converge on multimodal association areas in the prefrontal, the parietotemporal, and limbic cortices. (The limbic cortices form an unbroken stretch along the medial edge of the hemisphere, surrounding the corpus callosum and the diencephalon.) Orange = somatosensory association cortex; purple = visual association cortex; yellow = auditory association cortex. Sensory Information From Unimodal Areas of Cortex Converges in Multimodal Areas Sensory pathways dedicated solely to visual, auditory, or somatic information converge in multimodal association areas in the prefrontal, parietotemporal, and limbic cortices (Figure 19-4). Neurons in these areas respond to combinations of signals representing different sensory modalities by constructing an internal representation of the sensory stimulus concerned with a specific aspect of behavior. For example, the multimodal sensory association cortex in the inferior parietal lobule is concerned with directing visual attention to objects in the contralateral visual field. Neurons in this area receive information about the position of a stimulus in the world as well as its spatial relationship to the individual's personal space. In monkeys, neurons in this area may respond to sight of a reward if the reward is within arm's reach (personal space) but not if it is across the room (extra-personal space). These neurons also receive highly specific information from the cingulate cortex (the limbic association area), such that emotional state is a factor in their firing. For example, if a monkey is presented with a syringe filled with juice, neurons in the inferior parietal lobule may respond more vigorously if the monkey is thirsty than if it is sated. .
- Figure 19-12 Common output targets of parietal and prefrontal association areas in cortical and subcortical areas. The connections of the posterior parietal (intraparietal sulcus) and caudal principal sulcus are based on double-label studies in which one anterograde tracer was injected into the prefrontal cortex and another into the parietal cortex of the same animal. Superimposition of adjacent sections shows these areas projecting to common target areas including (1) limbic areas on the medial surface, (2) opercular and superior temporal cortices on the lateral surface, and (3) a range of subcortical sites. (Adapted from Goldman-Rakic 1987.) Interaction Among Association Areas Leads to Comprehension, Cognition, and Consciousness The dorsolateral prefrontal association cortex and parietal association cortex are among the most densely interconnected regions of association cortex, and both project to numerous common cortical and subcortical structures (Figure 19-12). The interactions between the posterior and anterior association areas are critical in guiding behaviors. Neurons in the posterior association areas often also continue firing after the stimulus has ceased. They may also respond to a particular stimulus only when the stimulus is involved in a behavior, and not when the stimulus is not involved. For example, they might fire in response to a light if it is a cue to explore the nearby space (to obtain a reward). These neurons fire regardless of the type of behavioral response required, such as an eye or hand movement, and may even fire when the animal is prevented from making any exploratory movement but merely required to attend to a part of space from the periphery of its vision to obtain a reward. Hence, neurons in the posterior association area are most tightly linked to the sensory rather than motor aspects of a complex behavior. Neurons in the premotor cortex may have similarly selective responses to sensory stimuli, but they fire only if action (motor output) is required. The interactions between the posterior and anterior association areas determine whether an action will occur and what the temporal pattern of motor responses will be. More than a century ago John Hughlings Jackson expressed the view that the conscious sense of a coherent self is not the outcome of a distinct system in the brain. Rather, he argued, consciousness emerges from the operation of the association cortices. Patients with focal lesions of association areas have selective and quite restricted loss of self-awareness for certain classes of stimuli while maintaining awareness for others. For example, a patient with a large lesion in the right (nondominant) parietal lobe may be unaware of the contralateral world. Lacking the concept of “left,” the patient will eat only the food on the right side of the tray and, if still hungry, will learn to rotate to the right in order to position the remaining food on the right side. Similarly, a patient with language disturbance resulting from damage to Wernicke's area will be unaware of the symbolic content of language. The patient will prattle on in response to a question, without understanding the question. Because the patient's “speech” is inflected normally with emotional tone, it appears from the patient's behavior as if words are merely an adornment to gestural communication. Similar dissociation is found in the so-called split-brain patient, in whom the cerebral hemispheres have been separated (by surgically sectioning the corpus callosum and anterior commissure) in order to control chronic epileptic seizures. Split-brain patients seem to have two independent conscious selves. Because the nondominant (usually right) hemisphere is “mute,” some might assume that only the dominant (left) hemisphere, which “talks,” is conscious. However, as we shall see next, by forcing behavioral choices that rely upon information available only to the right hemisphere, it is possible to identify a broad range of cognitive functions that are mediated by the right hemisphere alone.
- Affective Traits and Aspects of Personality Are Also Anatomically Localized Despite the persuasive evidence for localized languagerelated functions in the cortex, the idea nevertheless persisted that affective (emotional) functions are not localized. Emotion, it was believed, must be an expression of whole-brain activity. Only recently has this view been modified. Although the emotional aspects of behavior have not been as precisely mapped as sensory, motor, and cognitive functions, distinct emotions can be elicited by stimulating specific parts of the brain in humans or experimental animals. The localization of affect has been dramatically demonstrated in patients with certain language disorders and those with a particular type of epilepsy. Aphasia patients not only manifest cognitive defects in language, but also have trouble with the affective aspects of language, such as intonation (or prosody ). These affective aspects are represented in the right hemisphere and, rather strikingly, the neural organization of the affective elements of language mirrors the organization of the logical content of language in the left hemisphere. Damage to the right temporal area corresponding to Wernicke's area in the left temporal region leads to disturbances in comprehending the emotional quality of language, for example, appreciating from a person's tone of voice whether he is describing a sad or happy event. In contrast, damage to the right frontal area corresponding to Broca's area leads to difficulty in expressing emotional aspects of language. Thus some linguistic functions also exist in the right hemisphere. Indeed, there is now considerable evidence that an intact right hemisphere may be necessary to an appreciation of subtleties of language, such as irony, metaphor, and wit, as well as the emotional content of speech. Certain disorders of affective language that are localized to the right hemisphere, called aprosodias , are classified as sensory, motor, or conduction aprosodias, following the classification used for aphasias. This pattern of localization appears to be inborn, but it is by no means completely determined until the age of about seven or eight. Young children in whom the left cerebral hemisphere is severely damaged early in life can still develop an essentially normal grasp of language. Further clues to the localization of affect come from patients with chronic temporal lobe epilepsy. These patients manifest characteristic emotional changes, some of which occur only fleetingly during the seizure itself and are called ictal phenomena (Latin ictus , a blow or a strike). Common ictal phenomena include feelings of unreality and déjàvu (the sensation of having been in a place before or of having had a particular experience before); transient visual or auditory hallucinations; feelings of depersonalization, fear, or anger; delusions; sexual feelings; and paranoia. More enduring emotional changes, however, are evident when patients are not having seizures. These interictal phenomena are interesting because they represent a true psychiatric syndrome. A detailed study of such patients indicates they lose all interest in sex, and the decline in sexual interest is often paralleled by a rise in social aggressiveness. Most exhibit one or more distinctive personality traits: They can be intensely emotional, ardently religious, extremely moralistic, and totally lacking in humor. In striking contrast, patients with epileptic foci outside the temporal lobe show no abnormal emotion and behavior. One important structure for the expression and perception of emotion is the amygdala, which lies deep within the cerebral hemispheres. The role of this structure in emotion was discovered through studies of the effects of the irritative lesions of epilepsy within the temporal lobe. The consequences of such irritative lesions are exactly the opposite of those of destructive lesions resulting from a stroke or injury. Whereas destructive lesions bring about loss of function, often through the disconnection of specialized areas, the electrical storm of epilepsy can increase activity in the regions affected, leading to excessive expression of emotion or over-elaboration of ideas. We consider the neurobiology of emotion in Part VIII of this book.
- B. Left Parietal Lobe Syndrome: 1. Gerstmann Syndrome: acalculia, finger agnosia, left/right disorientation, agraphia. The lesion is in the left angular gyrus. Since there is often some degree of receptive aphasia and anomia, some features may be due to language disturbance. 2. Fluent aphasia, due to lesions of the temporal/parietal junction (i.e. Wernicke's, conduction, see Aphasic Disorders). 3. Alexia with agraphia can occur with angular gyrus lesions; some cases produce profuse semantic errors (i.e. deep dyslexia). 4. There are less severe deficits in constructional ability and milder forms of hemi-inattention to contralateral space.
- A. Right Parietal Lobe Syndrome: 1. Constructional apraxia is manifested by deficits in block design, stick design, drawing and geometric design. Patients tend to focus on individual elements (local properties) and lose the overall picture (global properties). This deficit extends to geographical space disorientation. 2. The hemi-inattention or hemi-neglect syndrome is the most dramatic non- dominant hemispheric syndrome and is seen in cortical lesions involving the temporal-parietal junction or the frontal eye field. Neglect can also be seen in unilateral thalamic lesions. The patient shows neglect of the contralateral half of visual space, the most severe example being anosognosia or denial of illness. Patients may deny having hemiplegia and may even deny the hemiparetic arm is theirs. Mild forms include extinction of the contralateral (left) stimulus during simultaneous presentation of bilateral visual, tactile or auditory stimuli. 3. Dressing apraxia - The patient has difficulty dressing the left side of body.
- Recording from single neurons in the brain of an awake, behaving rhesus monkey. (A) Lateral view of the rhesus monkey brain showing the parietal (red), temporal (green), and frontal (blue) cortices. The occipital cortex is shaded purple. (B) The animal is seated in a chair and gently restrained. Several months before data collection begins, a recording well is placed through the skull using a sterile surgical technique. For electrophysiological recording experiments, a tungsten microelectrode is inserted through the dura and arachnoid, and into the cortex. The screen and the response bar in front of the monkey are for behavioral testing. In this way, individual neurons can be monitored while the monkey performs specific cognitive tasks. Figure 26.10. Selective activation of neurons in the parietal cortex of a rhesus monkey during the fixation of a significant visual target (in this case, a spot of light associated with a food reward). (A) Region of recording. (B) Although the baseline level of activity of the neuron being studied here changes little in response to an uninteresting target (left), it increases its firing rate tenfold during eye fixation on a target of interest (right). The histograms indicate action potential frequency per unit time. (After Lynch et al., 1977.) “ Attention Neurons” in the Monkey Parietal Cortex These clinical and pathological observations clearly indicate distinct cognitive functions for the parietal, temporal, and frontal lobes. They do not, however, provide much insight into how the nervous system represents this information in nerve cells and their interconnections. The apparent functions of thea ssociation cortices implied by these clinical observations stimulated a number of informative electrophysiological studies in nonhuman primates, particularly macaque (usually rhesus) monkeys. As in humans, a wide range of cognitive abilities in monkeys are mediated by the association cortices of the parietal, temporal, and frontal lobes ( Figure 26.9A ). Moreover, these functions can be tested using behavioral paradigms that assess attention, identification, and planning capabilities, the broad functions respectively assigned to the parietal, temporal, and frontal association cortices in humans. Needless to say, it is far more practical to study neuronal behavior in relation to cognitive functions in experimental animals. Using implanted electrodes, recordings can be made from single neurons in the brains of awake, behaving monkeys to assess the activity of individual cells in the association cortices as various cognitive tasks are performed ( Figure 26.9B ). An example is neurons apparently related to the attentive functions of the parietal cortex. These particular studies of cellular electrophysiology and behavior take advantage of the fact that eye movements provide an excellent indicator of attentive behavior in primates. Thus, fixation of the eyes on a target the monkey has been trained to attend to can be used to identify attention-sensitive neurons in this part of the cortex ( Figure 26.10 ). As might be expected from the clinical evidence in humans, some neurons in specific regions of the parietal cortex of the rhesus monkey increase their rate of firing when the animal fixates on a target of interest, and they maintain their activity for the duration of the eye fixation. Responses of this sort are also observed when the monkey simply fixates on a test stimulus that has been associated with a food reward. When attention to the stimulus flags, eye movements resume, and the firing of the neurons falls to baseline levels. Thus, the monkey parietal cortex contains neurons that respond specifically when the animal attends to a behaviorally meaningful stimulus.
- . In confirmation of the impressions derived from neurological patients with parietal lobe damage, the right parietal cortex of normal subjects is highly active during tasks requiring attention. (A) A subject has been asked to attend to objects in the left visual field; only the right parietal cortex is active. (B) When attention is shifted from the left visual field to the right, the right parietal cortex remains active, but activity is apparent in the left parietal cortex as well. This arrangement implies that damage to the left parietal lobe does not generate right-sided hemineglect because the right parietal lobe also serves this function. (After Posner and Raichle , 1994 .)
- Characteristic performance on visuospatial tasks by individuals suffering from contralateral neglect syndrome. In (A), the patient was asked to draw a house by copying the figure on the left; on the right is the subject's imitation. In (B), the patient was asked to bisect the line. (C) Sequential self-portraits made by the artist Anton Raederscheidt over the period of his recovery from a right parietal stroke, showing progressive improvement in his attention to the left side of his mirror image. (A,B adapted from Posner and Raichle , 1994 ; C from Jung, 1974.) The location of the underlying lesions in eight patients diagnosed with contralateral neglect syndrome. (A) The site of damage was ascertained from CT scans (see Box B in Chapter 1 ). The lesions shown in 1–5 include parietal cortical areas (and in some cases, frontal areas). The lesions in 6–8, however, are mainly in the temporal lobe of the right hemisphere. These cases may reflect disruption of the pathways to and from the parietal cortex to other relevant brain areas. (B) Composite of these cases indicates the region (dotted line) of the right parietal lobe that is most often affected. (After Heilman and Valenstein , 1985 .) Lesions of the Parietal Association Cortex: Deficits of Attention In 1941, the British neurologist W. R. Brain reported three patients with unilateral parietal lobe lesions in whom the primary problem was varying degrees of perceptual difficulty. Brain described their peculiar deficiency in the following way: Though not suffering from a loss of topographical memory or an inability to describe familiar routes, they nevertheless got lost in going from one room to another in their own homes, always making the same error of choosing a right turning instead of a left, or a door on the right instead of one on the left. In each case there was a massive lesion in the right parieto-occipital region, and it is suggested that this … resulted in an inattention to or neglect of the left half of external space. The patient who is thus cut off from the sensations which are necessary for the construction of a body scheme may react to the situation in several different ways. He may remember that the limbs on his left side are still there, or he may periodically forget them until reminded of their presence. He may have an illusion of their absence, i.e. they may ‘feel absent' although he knows that they are there; he may believe that they are absent but allow himself to be convinced by evidence to the contrary; or, finally, his belief in their absence may be unamenable to reason and evidence to the contrary and so constitute a delusion. W. R. Brain, 1941 ( Brain 64: pp. 257 and 264) This description is generally considered the first account of the link between parietal lobe lesions and deficits in attention or perceptual awareness. Based on a large number of patients studied since Brain's pioneering work, these deficits are now referred to as contralateral neglect syndrome . The hallmark of contralateral neglect is an inability to perceive and attend to objects, or even one's own body, in a part of space, despite the fact that visual acuity, somatic sensation, and motor ability remain intact. Affected individuals fail to report, respond to, or even orient to stimuli presented to the side of the body (or visual space) opposite the lesion ( Figure 26.5 ). They may also have difficulty performing complex motor tasks on the neglected side, including dressing themselves, reaching for objects, writing, drawing, and, to a lesser extent, orienting to sounds. The signs of neglect can be as subtle as a temporary lack of contralateral attention that rapidly improves as the patient recovers, or they can be as profound as permanent denial of the existence of the side of the body and extrapersonal space opposite the lesion. Since Brain's original description of contralateral neglect and its relationship to lesions of the parietal lobe, it has been generally accepted that the parietal cortex, particularly the inferior parietal lobe, is the primary cortical region (but not the only region) governing attention ( Figure 26.6 ). Importantly, contralateral neglect syndrome is specifically associated with damage to the right parietal cortex. The unequal distribution of this particular cognitive function between the hemispheres is thought to arise because the right parietal cortex mediates attention to both left and right halves of the body and extrapersonal space, whereas the left hemisphere mediates attention only to the right. Thus, left parietal lesions tend to be compensated by the intact right hemisphere. In contrast, when the right parietal cortex is damaged, there is little or no compensatory capacity in the left hemisphere to mediate attention to the left side of the body or extrapersonal space. This interpretation has been confirmed by noninvasive imaging of parietal lobe activity during specific attention tasks carried out by normal subjects. Such studies show that blood flow is increased in both the right and left parietal cortices when subjects are asked to perform tasks in the right visual field requiring selective attention to distinct aspects of a visual stimulus such as its shape, velocity, or color. However, when a similar challenge is presented in the left visual field, only the right parietal cortex is activated. Moreover, when normal subjects are asked to maintain a state of general alertness, the right parietal cortex is especially active ( Figure 26.7 ). There is also evidence of increased activity in the right frontal cortex during such tasks (see also Figure 26.6 ). This latter observation suggests that, at least to some extent, regions outside the parietal lobe also contribute to attentive behavior, and perhaps to some aspects of the pathology of neglect syndromes. Overall, however, metabolic mapping is consistent with the clinical fact that contralateral neglect typically arises from a right parietal lesion, and it endorses the broader idea that there is hemispheric specialization for attention, just as there is for a number of other cognitive functions (see Chapter 27 ). Interestingly, patients with contralateral neglect are not simply deficient in their attentiveness to the left visual field, but to the left sides of objects generally. For example, in tasks in the right visual field, patients more readily identify novel stimuli on the right side of any object, wherever it happens to be in the right visual field. This observation suggests that attentiveness to objects is predicated on their “centroids,” and that the relevant frame of reference in neglect is at least in part object-based.
- Left Temporal Primary functions of this lobe include: decoding of speech sounds, comprehension of speech and mediating verbal memory processes. A. Dysfunctions associated with lesions of the left temporal lobe. Auditory deficits (right ear) Intracranial localization of sound is impaired. Increased threshold for perception of short bursts of sound. Increased threshold for some frequencies. Failure to perceive brief simultaneous auditory stimulation. Visual deficit (both eyes) Upper right quadrantanopsia. Other complex sensory deficits Right hand tactile performance difficulty. Right hand finger agnosia.
- Language deficits Decoding of speech sounds (phonemes) is impaired. Problems with verbal repetition. Problems with auditory comprehension of speech. Receptive aphasia (deficits in all language qualities). Impairment of dichotic listening to verbal material. Intellectual impairment on verbally mediated intellectual processes. Memory impaired for verbal material. Impairment on measures of higher cortical functions (Trails A and Trails B). Emotional disturbances Perceptual distortions, alterations of mood, obsessional thinking, psychosis, temper outbursts, hypo and hypersexuality.
- Figure 26.11. Selective activation of face cells in the inferior temporal cortex of a rhesus monkey. (A) Region of recording. (B) The neuron being recorded from here responds selectively to faces seen from the front. Scrambled parts of faces (stimulus 2) or faces with parts omitted (stimulus 3) do not elicit a maximal response. The cell responds best to different monkey faces, as long as they are complete and viewed from the front (stimulus 4); the cell also responds to a bearded human face (stimulus 5), although not quite as robustly. An irrelevant stimulus (in this case a hand; stimulus 6) does not elicit a response. (C) In this case, the neuron being recorded from responds to profiles of faces. A face viewed from the front (stimulus 1), 30° (stimulus 2), or 60° (stimulus 3) is not as effective as a true profile (stimulus 4). The cell will respond to profiles of different monkeys (stimulus 5), but is unresponsive to an irrelevant stimulus (in this case a brush; stimulus 6). (After Desimone et al., 1984.) “ Recognition Neurons” in the Monkey Temporal Cortex In keeping with human deficits of recognition following temporal lobe lesions, neurons with responses that correlate with the recognition of specific stimuli are present in the temporal cortex of rhesus monkeys ( Figure 26.11 ). The behavior of these neurons in the vicinity of the inferior temporal gyrus is generally consistent with one of the major functions ascribed to the human temporal cortex—namely, the recognition and identification of complex stimuli. For example, some neurons in the inferior temporal gyrus of the rhesus monkey cortex respond specifically to the presentation of a monkey face. These cells are generally selective; thus, some respond only to the frontal view of a face and others only to profiles ( Figure 26.11B , C ). Furthermore, the cells are not easily deceived. When parts of faces or generally similar objects are presented, such cells typically fail to respond. In principle, it is unlikely that such “face cells” are tuned to specific faces or objects, and no cells have so far been found that are selective for a particular face. However, it is not hard to imagine that populations of neurons differently responsive to various features of faces or other objects could act in concert to enable the recognition of such complex sensory stimuli
- Functional brain imaging of temporal lobes during face recognition. (A) Face stimulus presented to a normal subject at time indicated by arrow. Graph shows activity change in the relevant area of the right temporal lobe. (B) Location of f MRI activity in right inferior frontal lobe. (Courtesy of Greg McCarthy.) Lesions of the Temporal Association Cortex: Deficits of Recognition Clinical evidence from patients with lesions of the association cortex in the temporal lobe indicate that one of the major functions of this part of the brain isrecognition and identification of stimuli that are attended to, particularly complex stimuli. Thus, damage to either temporal lobe can result in difficulty recognizing, identifying, and naming different categories of objects. These disorders, collectively called agnosias (from the Greek for “not knowing”), are quite different from the neglect syndromes. As noted, patients with right parietal lobe damage often deny awareness of sensory information in the left visual field (and are less attentive to the left sides of objects generally), despite the fact that the sensory systems are intact (for instance, an individual with contralateral neglect syndrome typically withdraws his left arm in response to a pinprick, even though he may not admit the arm's existence). Patients with agnosia, on the other hand, acknowledge the presence of a stimulus, but are unable to report what it is. These latter disorders have both a lexical aspect (a mismatching of verbal or cognitive symbols with sensory stimuli; see Chapter 27 ) and a mnemonic aspect (a failure to recall stimuli when confronted with them again; see Chapter 31 ). One of the most thoroughly studied agnosias following damage to the temporal association cortex in humans is the inability to recognize and identify faces. This disorder, called prosopagnosia ( prosopo -, from the Greek for “face” or “person”), was recognized by neurologists in the late nineteenth century and remains an area of intense investigation. After damage to the temporal lobes, typically the right temporal lobe, patients are often unable to identify familiar individuals by their facial characteristics, and in some cases cannot recognize a face at all. Nonetheless, such individuals are perfectly aware that some sort of visual stimulus is present and can describe particular aspects or elements of it without difficulty. An example is the case of L.H., a patient described by the neuropsychologist N. L. Etcoff and colleagues in 1991 . (The use of initials to identify neurological patients in published reports is standard practice.) This 40-year-old minister and social worker had sustained a severe head injury as the result of an automobile accident when he was 18. After recovery, L.H. could not recognize familiar faces, report that they were familiar, or answer questions about faces from memory. He was nonetheless able to lead a fairly normal and productive life. He could still identify other common objects, could discriminate subtle shape differences, and could recognize the sex, age, and even the “likability” of faces. Moreover, he could identify particular people by nonfacial cues such as voice, body shape, and gait. The only other category of visual stimuli he had trouble recognizing was animals and their expressions, though these impairments were not as severe as for human faces. Noninvasive brain imaging showed that L.H.'s prosopagnosia was the result of damage to the righttemporal lobe. More recently, imaging studies in normal subjects have confirmed that the inferior temporal lobe mediates face recognition and that nearby regions are responsible for categorically different recognition functions ( Figure 26.8 ). In general, lesions of the right temporal lobe lead to agnosia for faces and objects, whereas lesions of the corresponding regions of the left temporal lobe tend to result in difficulties with language-related material (recall that the primary auditory cortex is on the superior aspect of the temporal lobe; as described in the following chapter, the cortex adjacent to the auditory cortex in the lefttemporal lobe is specifically concerned with language). The lesions that typically cause recognition deficits are in the inferior temporal lobe in or near the fusiform gyrus (those that cause language-related problems in the left temporal lobe tend to be on the lateral surface of the lobe). Consistant with these conclusions, electrical stimulation in subjects whose temporal lobes are being mapped for neurosurgery (typically removal of an epileptic focus) may have a transient prosopagnosia as a consequence of this abnormal activation of the relevant regions of the right temporal lobe. Prosopagnosia and related agnosias involving objects are specific instances of a broad range of functional deficits that have as their hallmark the inability to recognize a complex sensory stimulus as familiar, and to identify and name that stimulus as a meaningful entity in the environment. Depending on the laterality, location, and size of the lesion in temporal cortex, agnosias can be as specific as for human faces, or as general as an inability to name most familiar objects.